
Update on Broken Aids
Friday, September 25, 2009
I cannot express the great sense of appreciation that I feel for our new audiologist at Children's. She is a wonderful asset and she is already an incredible advocate for our little girl. We received a call from her Wednesday night that she had news-both good and bad. She had consulted with a few other audiologists and everyone agreed that Abby's hearing aids were simply not powerful enough to allow her to hear all the different frequencies of speech. This conclusion was based on the results of Abby's second ABR, which indicated that her residual hearing levels were 10 decibels less than her original diagnosis. Her current aids were being maxed out and still could not reach the highest frequency speech sounds--what this means is that even at their max power her aids would not allow her to distinguish between "sail" and "pail." Since our insurance only pays for hearing aids once every 3 years and the aids that she was recommending were $800 more expensive than her original ones, she was prepared to tell us that we will have to pay out of pocket for the upgrade.
However, she felt that these new aids were really what Abby has needed from day one and that it was not our fault that she was not given the equipment that she truly needed. Our insurance would have paid for these more expensive aids in the beginning, but since we had already filed a claim for her original aids we were pretty much out of luck. Our audiologist was not ready to accept this and agreed that we should not be held responsible for the audiological care that had failed Abigail. She called the rep from Oticon (the company that manufactured Abby's hearing aids) and was able to work a deal between Dayton Children's and Oticon to refund the original order and replace them with brand new, more powerful aids.
We feel so blessed to have such a wonderful professional on our team!
However, she felt that these new aids were really what Abby has needed from day one and that it was not our fault that she was not given the equipment that she truly needed. Our insurance would have paid for these more expensive aids in the beginning, but since we had already filed a claim for her original aids we were pretty much out of luck. Our audiologist was not ready to accept this and agreed that we should not be held responsible for the audiological care that had failed Abigail. She called the rep from Oticon (the company that manufactured Abby's hearing aids) and was able to work a deal between Dayton Children's and Oticon to refund the original order and replace them with brand new, more powerful aids.
We feel so blessed to have such a wonderful professional on our team!
I can't believe it!
Thursday, September 10, 2009
Today was a stressful day. I decided to run a few loads of laundry while the kids were playing nicely together in the toy room. After a few minutes Abby started screaming. I rushed in to see what was wrong and there was Benjy trying to hold her back by the elastic strap of her hearing aid clip. I have seen him do this a few times before and each time he has been reprimanded swiftly for it. I was just about to yell, "Let Go!," when I saw it happen. The elastic clip snapped, her hearing aid flew up in the air while the ear hook (the plastic part of the hearing aid that the earmold is connected to)was still attached to her ear mold. He had pulled so hard that the whole thing cracked right in half! I screamed--partly because I wasn't sure if he would live to see dinnertime and partly because I had no idea what else to do. I couldn't believe it--a three year old managed to break a fifteen-hundred dollar piece of equipment in the blink of an eye and even worse, right in front of me.
I spent the next thirty minutes on the phone with our new audiologist figuring out the next step. Lucky for us Oticon (the company that manufactured Abby's aids) warrants the hearing aids for one year--no matter what. The means that if Abby throws them out the window on the interstate--they'll replace them, or if in our case her brother decides she's a horse and can be controlled with her built-in "reins" and the aid splits right in half--they'll replace them. Thank God we're still in the warranty period. We will have to make an unexpected trip back down to Cincinnati tomorrow to fill out our warranty paperwork, send the broken aids in (we are going to send both in to be checked and/or replaced) and fit a set of loaner aids for Abby. Most pediatric audiology departments run a loaner program for this exact purpose. Her loaner aids will be programmed to her loss and will help her to stay on track while we wait the two-three weeks for her aids to be repaired.
As I type this I am sad, looking down at this pearl pink hearing aid cracked in half. Her aids are as much a part of her as her big blue eyes and I wonder how lonely she must feel when she can't hear our voices.
I spent the next thirty minutes on the phone with our new audiologist figuring out the next step. Lucky for us Oticon (the company that manufactured Abby's aids) warrants the hearing aids for one year--no matter what. The means that if Abby throws them out the window on the interstate--they'll replace them, or if in our case her brother decides she's a horse and can be controlled with her built-in "reins" and the aid splits right in half--they'll replace them. Thank God we're still in the warranty period. We will have to make an unexpected trip back down to Cincinnati tomorrow to fill out our warranty paperwork, send the broken aids in (we are going to send both in to be checked and/or replaced) and fit a set of loaner aids for Abby. Most pediatric audiology departments run a loaner program for this exact purpose. Her loaner aids will be programmed to her loss and will help her to stay on track while we wait the two-three weeks for her aids to be repaired.
As I type this I am sad, looking down at this pearl pink hearing aid cracked in half. Her aids are as much a part of her as her big blue eyes and I wonder how lonely she must feel when she can't hear our voices.
What does Abby's loss sound like?
Wednesday, September 9, 2009
This video is a great way to understand Abigail's hearing loss. The first time I saw this I cried because it made Abby's loss real to me. I finally understood what life for her would be like without her aids. While her hearing aids will help her greatly in understanding and developing speech, she will still struggle. It will be hard for her to understand you unless you are talking in front of her; in a crowded room that is noisy it will be almost impossible for her to distinguish your voice from the other noises in the room and she will have to work very hard and train her ears to hear the difference between the highest frequency sounds such as "s" and "sh."
As you watch this video you will see the audiogram in the lower right hand corner shift from mild loss to moderate loss to severe loss. Abigail has severe (65-75 dB loss) bilateral (both ears) sensorineural (nerve damage) hearing loss and this is what we sound like to her.
As you watch this video you will see the audiogram in the lower right hand corner shift from mild loss to moderate loss to severe loss. Abigail has severe (65-75 dB loss) bilateral (both ears) sensorineural (nerve damage) hearing loss and this is what we sound like to her.
Abby's Second ABR Results

The day started out rough--we had a terrible storm the night before and the roads were very foggy in the morning. The kids were packed and we were ready to head out at about 7 am. Abigail wasn't allowed to have anything at all after 7 am, but was allowed to have about 4 oz of clear juice at 6 am. This made for a very hungry little girl on the almost 2 hour trip to Cincinnati (I hate rush hour traffic.) Of course it didn't help that her brother was drinking chocolate milk and eating glazed donut holes two feet from her.
We finally arrived and after an hour of paperwork (she had to be checked out by a couple of additional doctors because of her heart murmur--she is going to see a pediatric cardiologist next week) she was given the sedative. Benjy watched Lion King while I tried to rock Abby asleep. She was doing really well until she started to feel the effects of the medicine. That loss of control over her body really seemed to scare her and she began to totally freak out. After ten or fifteen minutes of trying to hold on to her, I called the nurses in to help me. We decided that the best thing to do was to wrap her in a blanket from the warmer and simply hold her down until she fell asleep. This was hard for me because she was screaming so loud, but if she didn't fall asleep with the sedative they would have to use general anesthesia.
The audiologist eased my mind a bit and explained that this sort of reaction is very common among kids with hearing loss. Since their hearing is impaired, their other senses are often heightened. This makes them especially sensitive to changes in their other senses and they can experience anxiety when they feel another sense has been impaired. After about twenty minutes of screaming she finally gave in and fell asleep. About 45 minutes later the audiologist brought us a new audiogram that accurately established the degree of her loss.
It turns out that while her first ABR indicated a moderate/moderate-severe loss and subsequent hearing tests had produced a mild/moderate loss result, her actual loss fell in the severe range. Her audiogram shows that without her aids she is not able to hear any of the sounds of speech and in fact she is unable to hear most normal conversations (typically occurs at 50 dB) without her aids. I was disappointed; not because her loss was more severe than we had originally thought, but that we had already wasted a year with poor programming for her aids.
Our First Trip to Cincinnati
Friday, September 4, 2009
Yesterday was our first appointment with our new Audiologist at the Mason campus of Cincinnati Children's Hospital. We decided to leave Dayton Children's after a series of mistakes were made:
We are quite nervous about sedating her, but know that this is a necessary step to her speech development. We feel confident that moving to Cincinnati Children's was a step in the right direction. We feel like we learned more from this two hour appointment than we have learned from an entire year of care at Dayton Children's. Our course of action is as follows:
- Abigail's hearing aids have a rocker switch that controls the volume. For kids under the age of four, this switch is supposed to be disabled via the computer software that initially programs the aids. After eight months and two trips to see two different audiologists regarding the programming of her aids, we discovered that her volume controls were never disabled. Each time we cleaned her aids we were unknowingly raising and lowering the volume--a lot of very precious hearing time wasted.
- Three different requests to have ear molds redone because of audiologist error.
- The inability for our original ENT to explain our Connexin 26 diagnosis to us.
- The polite refusal to repeat a hearing test because I thought her last test was not accurate.
We are quite nervous about sedating her, but know that this is a necessary step to her speech development. We feel confident that moving to Cincinnati Children's was a step in the right direction. We feel like we learned more from this two hour appointment than we have learned from an entire year of care at Dayton Children's. Our course of action is as follows:
- Repeat Abby's ABR to determine exactly what her loss is;
- reprogram her hearing aids based on her new results; and
- meet with an Aural Rehabilitation Therapist to have an evaluation.
Abigail Turns One
Saturday, August 29, 2009

Happy birthday to our dear little princess!
It's hard to imagine that you're one today--it seems just like yesterday that we welcomed you into our family. While it doesn't seem like we've already been blessed with you for an entire year, it has been a long journey. We will remember forever the first time we saw you, your first tear, your first smile, your first laugh, your first kiss. We will remember forever the first time we learned that you had a hearing loss--the fears that we had, the tears that were shed, the many questions that would follow. We've come a long way as a family and your smiles have given us all the strength to keep going. We hope that you will one day understand the decisions we have made and know that we are working as hard as we can to make sure you have every tool possible to succeed and be happy
.
Can I get a mmmmmm.
Friday, August 7, 2009
We have been working diligently to encourage Abigail to increase the kinds of sounds that she is making, but still have not heard any of the typical consonant sounds that you hear from a baby her age. One of the first sounds that you can expect is the "b" sound, perhaps in the form of "ba" to refer to her bottle. Shortly after that the "d" for "da da" and the "m" for "ma" appear and before you know it your little one is speaking jargon (which I recently learned is an actual technical term for that period of time when your baby babbles with such inflection and tone that it sounds like she's having a conversation in a foreign language.) I have been plugging away at momma, but I would settle for a "ba" or even a "da" at this point. While she has progressed developmentally in some areas of speech--she has engaged in repetitive sounds (the ah ah ah sequence) and in back and forth style verbal play--she is still exhibiting a true speech delay.
We will be able to start medical model speech therapy (this is the type of speech therapy where the therapist actually works directly with Abigail to stimulate speech sounds, while the consultative approach consists more of the therapist providing suggestions to Ben and I on how to encourage her speech at home) in just a few weeks when Abby turns one. I am trying to decide on where to start her speech therapy. There are a few local outpatient centers here that I can try, but much like everything else in this process we are totally new to this and I'm not sure how to know if I've chosen a good speech therapist or not. Luckily my sister-in-law is very versed in speech therapy (she has a little boy with Apraxia) and she was able to provide me with some great guidelines:
We will be able to start medical model speech therapy (this is the type of speech therapy where the therapist actually works directly with Abigail to stimulate speech sounds, while the consultative approach consists more of the therapist providing suggestions to Ben and I on how to encourage her speech at home) in just a few weeks when Abby turns one. I am trying to decide on where to start her speech therapy. There are a few local outpatient centers here that I can try, but much like everything else in this process we are totally new to this and I'm not sure how to know if I've chosen a good speech therapist or not. Luckily my sister-in-law is very versed in speech therapy (she has a little boy with Apraxia) and she was able to provide me with some great guidelines:
- A good speech therapist should have a theory and process that he/she is able to explain to you regarding your child--this is the most important quality.
- The speech therapist should explain how you can continue what he/she is doing during the session at home.
- The speech therapist should be open and receptive to any ideas/concerns that you have regarding your child.
Working on signs
Sunday, August 2, 2009
Incorporating sign language into our daily routine has been very difficult for us as a family. After using only our voices to communicate for roughly the past 29 years, Ben and I have to really work on signing to Abigail. Remembering to do this is one of the most difficult hurdles we have to overcome. While our signing vocabulary is expanding every day, we still are not signing to each other or to Benjy regularly. We often forget to use our signs in key teaching moments like at dinner or bath. Our hearing therapist and deaf mentor had some great ideas that we are going to implement over the next week to help us get comfortable with signing:
- Establish a quiet time at dinner--even if just for ten minutes use only your signs to communicate. If this means all you say is please and thank you or dinner's good--that's fine. Abigail's first language is visual and she will be focused intently on your visual communication.
- Put of sign flash cards in various areas of the house that can serve as key teaching areas for both Abby and Benjy--the bath, the play room, the dinner table, the mudroom. Each area can emphasize 1 or 2 signs to start and the cards will serve as reminders to use our signs as well as our voices to communicate.
- Sign to each other and to your family--if you don't know a word, oh well! The more you practice, the more natural signing will become to you.
Deaf Mentor Services
Wednesday, July 29, 2009
This past week we had the first meeting with our new Deaf Mentor here in Ohio. We received deaf mentor services in Pittsburgh while Ben was deployed and I thought that the help and guidance that I received was vital. Since returning to Ohio not only have I missed these services, but also I feel that we would really be able to benefit since our family is whole again. RIHP (Regional Infant Hearing Program) was able to connect us with a new deaf mentor and we have services up and running again. I would highly recommend obtaining this service if it available to you--it plays a key role in introducing your family to the deaf community. Since we are a hearing family, we knew next to nothing about deaf culture or about what life is like when you're deaf, what life will be like for Abigail. There are no wrong or inappropriate questions when it comes to your deaf mentor--just answers, answers for anything that we as hearing parents might wonder about.
I learned so many things that I had never even thought of, but probably the most important thing that I learned was that I didn't have to be scared of the deaf community. It didn't matter that I was just learning ASL, it didn't matter that I still talked while I signed and it didn't matter that we were hearing and they were deaf. Everyone that I met was so eager to find out about our family and we were so eager to find out about others.
Some people have questioned our decision to become involved with the deaf community since Abigail isn't really deaf, she's hard of hearing. My response to that is that she's not really hearing either, she's hard of hearing. We believe that she should be involved with both the hearing community and the deaf community because she falls somewhere in between. We could decide not to teach her sign language, we could decide not to take her to deaf community events, we could decide to ignore the fact that she has a hearing loss altogether. But it still wouldn't change the fact that she has a hearing loss and as her parents we want to provide her with every tool possible so that she can succeed.
I learned so many things that I had never even thought of, but probably the most important thing that I learned was that I didn't have to be scared of the deaf community. It didn't matter that I was just learning ASL, it didn't matter that I still talked while I signed and it didn't matter that we were hearing and they were deaf. Everyone that I met was so eager to find out about our family and we were so eager to find out about others.
Some people have questioned our decision to become involved with the deaf community since Abigail isn't really deaf, she's hard of hearing. My response to that is that she's not really hearing either, she's hard of hearing. We believe that she should be involved with both the hearing community and the deaf community because she falls somewhere in between. We could decide not to teach her sign language, we could decide not to take her to deaf community events, we could decide to ignore the fact that she has a hearing loss altogether. But it still wouldn't change the fact that she has a hearing loss and as her parents we want to provide her with every tool possible so that she can succeed.
Results of the Developmental Assessment
Monday, July 20, 2009
We recently had our IFSP and received the written reports from the various evaluators that were present during Abby's assessment. The physical therapist determined that there was really no concerns about her gross or fine motor skills and that her size was probably the biggest inhibitor to her crawling. (She's a large baby who likes to eat!) The speech therapist and the EI both confirmed our thoughts that she did have a speech delay-approximately a two month delay. Although this might have been expected for a baby with hearing loss, it is certainly not what we strive for and she will be held to the same communicative milestones of a hearing baby. The major concern for her speech development was her failure to babble--i.e. no repetitive sounds like ah ah ah, no consonant sounds, and no back and forth "game-like" communication. Why this might sound silly, these beginning sounds are the basis for compound sounds, then identifying sounds, and so on and so forth.
The speech therapist gave us a Nuk brush to stimulate her tongue and mouth in hopes that this will lead to a greater production of sounds. We also are going to continue to encourage the "back and forth" game play with a variety of sounds. One of the things that Ben and I learned during this IFSP is that any signs that she learns to use will count toward the "15 by 15" count. (This is a very general guideline that a toddler should use 15 words or signs to communicate by 15 months.) We are going to continue to sign to her regularly and will begin medical model speech therapy at about 12 months.
So, the IFSP conclusion...
The speech therapist gave us a Nuk brush to stimulate her tongue and mouth in hopes that this will lead to a greater production of sounds. We also are going to continue to encourage the "back and forth" game play with a variety of sounds. One of the things that Ben and I learned during this IFSP is that any signs that she learns to use will count toward the "15 by 15" count. (This is a very general guideline that a toddler should use 15 words or signs to communicate by 15 months.) We are going to continue to sign to her regularly and will begin medical model speech therapy at about 12 months.
So, the IFSP conclusion...
- We will continue to have our hearing therapist meet with Abigail once a week;
- Our EI will come every other week to monitor Abby's progress in other areas of development;
- The speech therapist will come once a month to visit Abigail and provide us with ideas to encourage her communication;
- We will receive the services of a deaf mentor to help us build our sign language vocabulary and work on ways to incorporate signing into our daily lives; and
- We will begin medical model speech therapy at 12 months.
Developmental Assessment
Sunday, June 28, 2009
When we returned to Ohio and thus to Help Me Grow (Ohio's early intervention organization), we needed to have a second assessment done to identify how Abigail had progressed over the past six months. An assessment is a meeting between various professionals that will be involved with your child's care and your family. It is a chance for each of the professionals to observe and evaluate Abigail against their respective areas of development. Our assessment included a speech therapist, an early intervention specialist, a hearing therapist and a physical therapist (they're were some minor concerns that she had not started crawling yet.) Each professional evaluated Abigail while we discussed daily routines, Abigail's responses to family members, and any concerns that my husband and I had with her development.
Our EI (early intervention specialist) used the Hawaii Early Learning Program (HELP) charts to monitor Abigail's development, while the hearing and speech therapists used a variety of games to monitor both Abigail's verbal and non-verbal responses. The physical therapist conducted a variety of strength and balance tests to evaluate Abigail's motor skills. Each professional will be responsible for providing a copy of their findings reports at the IFSP. These reports will become part of the IFSP and serve as a baseline for future evaluation and comparison.
Our EI (early intervention specialist) used the Hawaii Early Learning Program (HELP) charts to monitor Abigail's development, while the hearing and speech therapists used a variety of games to monitor both Abigail's verbal and non-verbal responses. The physical therapist conducted a variety of strength and balance tests to evaluate Abigail's motor skills. Each professional will be responsible for providing a copy of their findings reports at the IFSP. These reports will become part of the IFSP and serve as a baseline for future evaluation and comparison.
Abigail's Second Hearing Test
Wednesday, June 10, 2009
Yesterday was Abigail's second hearing test in the sound booth. If you haven't ever experienced a pediatric hearing test, I will explain a little bit about how the test is done. The test is conducted in a soundproof room and usually requires the presence of two audiologists. There is one audiologist in the soundproof room with you and a second controlling the sound board (where the various tones and sounds are produced from). The idea behind the test is that if your child hears a tone, sound, etc. he/she will produce one of several reactions--a pause in play, raised eyes, or ideally they will look for the sound that they heard. This is why there is an audiologist that sits across from you--it is her job to monitor your child's reaction. If the child turns toward the side of the room where the sound originated they are rewarded by seeing a toy that was once hidden in darkness move and light up. The more sound booth tests that a child has taken, the more likely they are to search for which one of their friends (toys) made the noise.
Once I understood how these booth tests worked, I immediately questioned how accurate these tests actually were. It seems to me that there is a great deal of subjectivity in these tests--what one audiologist sees as a pause, another might not. In fact, how do we really know that her pause should be attributed to sound and not simply to gas. In this test it seemed like Abby was just searching for her friends (toys) and wasn't really paying attention to any tones at all. Since her first test had indicated that her loss may fall more in the mild to moderate loss range, I was eager for a second round of results to confirm this. Generally both aided and unaided tests are conducted in the sound booth--not only do we want to confirm that her hearing aids are functioning properly for her, but also we want to verify that her hearing hasn't degenerated at all. This test didn't seem to go so well and unfortunately we were only able to test her with her aids on. Our audiologist did not seem concerned and asked for us to come back in three months for a follow-up test.
At first I wasn't really concerned about it either, but the more I thought about it, the more I felt like I needed some sort of confirmation that her hearing loss hadn't gotten any worse. Her hearing aids were being programmed based on the first sound booth test that indicated she only had a mild-moderate loss, but she still wasn't babbling. I decided to call in and ask for a retest just to allay my fears that we might be missing something. I mean we already had wasted so much time because her hearing aid volume wasn't disabled, I didn't want to sit by and just accept something when I had such a bad feeling about it. Once again, it didn't seem to be a concern to my audiologist that she hadn't had an unaided test in six months. She again stated that she thought she would be fine until the October time frame and then we would do the unaided portion of the test first. Maybe it was because she hadn't seen Abigail since the beginning (we had worked with four different audiologists because of employee turnover since Abigail's initial diagnosis in October 2008), or maybe it was because I was too pushy. I am not sure, but for me it was the final straw--I had decided that we would transfer Abby's audiological care to Cincinnati Children's Hospital.
Once I understood how these booth tests worked, I immediately questioned how accurate these tests actually were. It seems to me that there is a great deal of subjectivity in these tests--what one audiologist sees as a pause, another might not. In fact, how do we really know that her pause should be attributed to sound and not simply to gas. In this test it seemed like Abby was just searching for her friends (toys) and wasn't really paying attention to any tones at all. Since her first test had indicated that her loss may fall more in the mild to moderate loss range, I was eager for a second round of results to confirm this. Generally both aided and unaided tests are conducted in the sound booth--not only do we want to confirm that her hearing aids are functioning properly for her, but also we want to verify that her hearing hasn't degenerated at all. This test didn't seem to go so well and unfortunately we were only able to test her with her aids on. Our audiologist did not seem concerned and asked for us to come back in three months for a follow-up test.
At first I wasn't really concerned about it either, but the more I thought about it, the more I felt like I needed some sort of confirmation that her hearing loss hadn't gotten any worse. Her hearing aids were being programmed based on the first sound booth test that indicated she only had a mild-moderate loss, but she still wasn't babbling. I decided to call in and ask for a retest just to allay my fears that we might be missing something. I mean we already had wasted so much time because her hearing aid volume wasn't disabled, I didn't want to sit by and just accept something when I had such a bad feeling about it. Once again, it didn't seem to be a concern to my audiologist that she hadn't had an unaided test in six months. She again stated that she thought she would be fine until the October time frame and then we would do the unaided portion of the test first. Maybe it was because she hadn't seen Abigail since the beginning (we had worked with four different audiologists because of employee turnover since Abigail's initial diagnosis in October 2008), or maybe it was because I was too pushy. I am not sure, but for me it was the final straw--I had decided that we would transfer Abby's audiological care to Cincinnati Children's Hospital.
Fast Forward...A lot!
Thursday, May 28, 2009
Well as you can see I have been somewhat sidetracked when it comes to this blog--maybe because in the last four months I have moved back to my house, welcomed my husband home from Iraq (yet again), left one early intervention program for another, undertaken a major home renovation, etc. It seems like I blinked and it was already time for fireworks! Since I haven't written in a while and now am so far behind in telling Abby's story, I am going to do a catch up post. So here goes...
Abigail has now been aided for 234 days (she was aided on November 6th at about 10 weeks.) For the first 215 days we were unknowingly operating the volume control (this feature was supposed to be disabled by our audiologist) and she would go through periods of crying and pulling them out repeatedly, which we have since attributed to the volume being way to loud and causing extreme discomfort for her little ears. I am quite displeased with our first audiologist who dismissed my early concerns that there was something wrong with the volume, however I am unable to voice my concerns since she conveniently moved just 1 week before discovering the problem. I hate the turnover in this industry, but I will reserve that for another post at a later date. We now have her aids up and running properly and she seems to be happy as a clam!
Her early blood tests indicated an elevated level of triglycerides and we were referred to a gastro doc to follow up. Our ENT explained that sometimes high levels of cholesterol can lead to hearing loss and we definitely want to preserve the residual hearing that she has. The gastro doc suspected that it was simply an inaccurate test result and reordered a second round of bloodwork. We recently met with our pediatrician who informed us that this second test also indicated a high cholesterol level and we are awaiting our follow-up with the gastro doc to discuss what exactly this means.
We moved back to our Ohio home in early May (my husband was deployed for 7 months to Iraq and we relocated to Pittsburgh) and started early intervention services back up. Abigail received a second developmental assessment at 9 months in preparation for a new IFSP to be created so that we could begin services as soon as possible. I will talk in my next post about the assessment and her new IFSP.
Abigail has now been aided for 234 days (she was aided on November 6th at about 10 weeks.) For the first 215 days we were unknowingly operating the volume control (this feature was supposed to be disabled by our audiologist) and she would go through periods of crying and pulling them out repeatedly, which we have since attributed to the volume being way to loud and causing extreme discomfort for her little ears. I am quite displeased with our first audiologist who dismissed my early concerns that there was something wrong with the volume, however I am unable to voice my concerns since she conveniently moved just 1 week before discovering the problem. I hate the turnover in this industry, but I will reserve that for another post at a later date. We now have her aids up and running properly and she seems to be happy as a clam!
Her early blood tests indicated an elevated level of triglycerides and we were referred to a gastro doc to follow up. Our ENT explained that sometimes high levels of cholesterol can lead to hearing loss and we definitely want to preserve the residual hearing that she has. The gastro doc suspected that it was simply an inaccurate test result and reordered a second round of bloodwork. We recently met with our pediatrician who informed us that this second test also indicated a high cholesterol level and we are awaiting our follow-up with the gastro doc to discuss what exactly this means.
We moved back to our Ohio home in early May (my husband was deployed for 7 months to Iraq and we relocated to Pittsburgh) and started early intervention services back up. Abigail received a second developmental assessment at 9 months in preparation for a new IFSP to be created so that we could begin services as soon as possible. I will talk in my next post about the assessment and her new IFSP.
Abby's First Booth Test
Wednesday, April 1, 2009
My mother-in-law and I headed back to Ohio for Abigail's first sound booth hearing test this past weekend. I had tried to schedule her hearing test, gastro appt. (for the high triglycerides that popped on her original bloodwork), genetic eval and ear molds all for the same day since we were coming from Pittsburgh. Everything went very smoothly, but I am slightly confused about her hearing test results. This new test indicated that Abigail only had a mild/moderate loss rather than the initial moderately-severe loss that her ABR (Auditory Brainstem Response) test showed. While I am incredibly happy that her loss is not as bad as we had originally thought, I am a bit concerned that we are going to be programming her hearing aids to correspond to these new results. The sound booth test is different than I expected and I am not sure how accurate it is. The entire test is based on subjective interpretation of Abby's reactions to sound. I will have to do some research to put my fears at ease, but for now I am cautiously happy about these results. I can't wait to tell Ben.
Below is a picture of a standard speech audiogram--the object pictures are placed on the audiogram where their typical sound decibel would be and the letters are representative of where those sounds would be in the speech banana. I have included a picture of Abigail's first hearing test audiogram as well so that you can understand exactly what we think she is hearing right now.

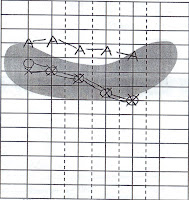
The A symbols refer to Abby's aided hearing (what she hears with her hearing aids on), the circle symbols refer to what she hears unaided with her right and the X refers to what she hears unaided with her left ear. The gray shaded banana shaped area is referred to as the speech banana--where most of the sounds of our speech exist. If she is able to hear above that speech banana, she should be able to develop speech normally. As you can see her aided results put her above the speech banana and just below the highest frequency sounds of "f," "s," "th."
Below is a picture of a standard speech audiogram--the object pictures are placed on the audiogram where their typical sound decibel would be and the letters are representative of where those sounds would be in the speech banana. I have included a picture of Abigail's first hearing test audiogram as well so that you can understand exactly what we think she is hearing right now.


The A symbols refer to Abby's aided hearing (what she hears with her hearing aids on), the circle symbols refer to what she hears unaided with her right and the X refers to what she hears unaided with her left ear. The gray shaded banana shaped area is referred to as the speech banana--where most of the sounds of our speech exist. If she is able to hear above that speech banana, she should be able to develop speech normally. As you can see her aided results put her above the speech banana and just below the highest frequency sounds of "f," "s," "th."
Abby's Hearing Aids are Finally In!
Saturday, March 14, 2009
Abigail's hearing aids came in just one week after our first ear mold impressions. Our audiologist had pre-programmed them specifically for Abigail's hearing loss and disabled the exterior volume button (so that Abigail wouldn't be able to turn them up/off accidentally). We arrived very eager and couldn't wait to see what they looked like, we were also very excited to see her reaction when she finally heard our voices for the first time! The audiologist spent almost an hour explaining our warranty, operation, how to care for the aids, etc. Oticon (the manufacturer of our hearing aids) will replace the hearing aids one time in the first year regardless of the cause of damage or loss. After that we were advised to talk to our home owners' insurance provider to see if we could set up some sort of rider on our policy to protect their loss. Since her hearing aids were $4000 and our health insurance only pays for a new pair once every four years, we need to have some sort of backup protection.
Our audiologist put them in for the first time and turned them on. Abigail seemed startled and started to cry. This made me really sad as I had expected giant smiles from this little two month old baby who was truly "hearing" for the first time. Our audiologist then took them out so that we could practice putting them in and taking them out by ourselves. It was really hard, I felt like I couldn't get the mold in her ear and they just kept whistling at me. The whistling was really surprising to us, I guess we never really understand how much feedback there would be when the aids were turned on. Feedback is a result of the sound that the aid amplifies leaking out of the inner ear and amplified a second time by the aid--it sounds similar to the feedback you sometimes hear on a microphone in an auditorium. Young babies are very susceptible to this feedback since they aren't able to support themselves yet--feedback is intensified by being too close to something or someone else (i.e. being held). The feedback was so bad that I left the office that day crying. My expectations were unrealistic. I did not expect that this new world of sound would be scary or annoying to her, I did not expect their to be so much work involved in caring for her aids and last but not least, I did not expect that their would be so much feedback for poor little ears.
I didn't know how I was going to do this, we had just left and I already hated her aids.
Our audiologist put them in for the first time and turned them on. Abigail seemed startled and started to cry. This made me really sad as I had expected giant smiles from this little two month old baby who was truly "hearing" for the first time. Our audiologist then took them out so that we could practice putting them in and taking them out by ourselves. It was really hard, I felt like I couldn't get the mold in her ear and they just kept whistling at me. The whistling was really surprising to us, I guess we never really understand how much feedback there would be when the aids were turned on. Feedback is a result of the sound that the aid amplifies leaking out of the inner ear and amplified a second time by the aid--it sounds similar to the feedback you sometimes hear on a microphone in an auditorium. Young babies are very susceptible to this feedback since they aren't able to support themselves yet--feedback is intensified by being too close to something or someone else (i.e. being held). The feedback was so bad that I left the office that day crying. My expectations were unrealistic. I did not expect that this new world of sound would be scary or annoying to her, I did not expect their to be so much work involved in caring for her aids and last but not least, I did not expect that their would be so much feedback for poor little ears.
I didn't know how I was going to do this, we had just left and I already hated her aids.
Let's get ear molds!
Friday, March 13, 2009
We went in for our first set of ear mold impressions and are getting even closer to getting Abigail's ears aided. We met with our audiologist to do the impressions and sign paperwork for the hearing aids. The process for taking the impressions was very quick. The audiologist took a small cotton ball attached to a string and pushed it into Abigail's ear canal, then used a two-part epoxy to fill her ear canal. The epoxy hardens very quickly, after only a few minutes, and is removed by the strings. The result is a perfect impression of the inside of Abigail's ear!
Our audiologist sends it off to Microsonic and we have ear molds in less than one week!
Ear molds come in many different colors including sparkles, confetti and bright neon colors. We chose to get lilac colored ear molds to match Abby's pink hearing aids.
Our audiologist sends it off to Microsonic and we have ear molds in less than one week!
Ear molds come in many different colors including sparkles, confetti and bright neon colors. We chose to get lilac colored ear molds to match Abby's pink hearing aids.
Our Questions Answered
Abigail's genetic profile came back on December 15, 2008. The tests revealed that Abigail's hearing loss is the result of a Connexin 26 gene mutation. Connexin 26 is a protein that helps different cells pass molecules between another, specifically it helps to cycle potassium through the cochlea and the inner ear. This results in a build-up of potassium and resulting nerve damage of the cochlea hair cells. In about 2/3 of patients this damage causes severe to profound hearing loss. In Abigail's case, she retained a greater amount of her hearing resulting in only a moderate-to-severe loss. Since this particular mutation is recessive, both my husband and I must be carriers to have passed the recessive trait on. We have no incidence of hearing loss on either side of our families and have an older child without hearing impairment.
Our question is finally answered--we have a reason. I was incredibly sad, but also relieved; sad that this was something that we had passed on and could potentially pass on to our other children, but also relieved to finally know that there was nothing that I did wrong--nothing that I could have done differently to prevent this. Since her hearing loss was determined to be genetic we were provided with an ENT that specialized in genetic hearing loss in addition to a geneticist.
Our question is finally answered--we have a reason. I was incredibly sad, but also relieved; sad that this was something that we had passed on and could potentially pass on to our other children, but also relieved to finally know that there was nothing that I did wrong--nothing that I could have done differently to prevent this. Since her hearing loss was determined to be genetic we were provided with an ENT that specialized in genetic hearing loss in addition to a geneticist.
State Funded Aid
The state of Ohio has an umbrella health care organization that exists to financially support all kids with medical handicaps, Bureau for Children with Medical Handicaps (BCMH). BCMH also provides support to special needs children that require ongoing medical treatments including diabetes, heart defects, chronic lung disease, cancer and hearing loss. The financial support is intended not only to help families without insurance, but also to supplement insurance to meet any co-pays or services not covered. This includes the cost of hearing aids and services associated with hearing loss.
While families must meet certain income requirements for treatment services, any and all diagnostic services are covered regardless of income. This means that any screenings, tests, x-rays, specialist appointments leading up to a diagnosis are covered 100% by BCMH. Your insurance will be the first payer, but any out of pocket costs will be picked up by BCMH. In addition BCMH provides extremely low-cost payment plans for hearing aids, public nurse visits and access to a variety of specialists.
I am not sure of state-funded organizations in different states as our experience is solely in Ohio. However, The National Dissemination Center for Children with Disabilities has an awesome website that allows you to search for agencies by state.
During that first meeting with our caseworker, we filled out the initial paperwork for BCMH to apply for financial support for diagnostic services. Within 4 weeks we received a letter of approval that we would be required to submit to all doctors or providers (i.e. children's hospitals, labs, etc.) that Abigail would be receiving care from.
While families must meet certain income requirements for treatment services, any and all diagnostic services are covered regardless of income. This means that any screenings, tests, x-rays, specialist appointments leading up to a diagnosis are covered 100% by BCMH. Your insurance will be the first payer, but any out of pocket costs will be picked up by BCMH. In addition BCMH provides extremely low-cost payment plans for hearing aids, public nurse visits and access to a variety of specialists.
I am not sure of state-funded organizations in different states as our experience is solely in Ohio. However, The National Dissemination Center for Children with Disabilities has an awesome website that allows you to search for agencies by state.
During that first meeting with our caseworker, we filled out the initial paperwork for BCMH to apply for financial support for diagnostic services. Within 4 weeks we received a letter of approval that we would be required to submit to all doctors or providers (i.e. children's hospitals, labs, etc.) that Abigail would be receiving care from.
The Question of Cost
I wanted to take a couple of posts to explain everything that we have learned about funding Abigail's treatment and hearing aids. This first post I will talk solely about the overall cost and insurance policies, while I will try to provide as much information about state-funded assistance programs in the next post.
Shortly after Abigail's HOH diagnosis we had a meeting with our caseworker to discuss our insurance and how we intended to fund the purchase of Abigail's hearing aids. Since Abigail has a bilateral loss (a hearing loss in both ears) we would be purchasing two hearing aids in addition to two ear molds (click here for an interesting article on ear molds). Hearing aids range in price from $1000 USD for a quality basic hearing aid to over $3000 USD for a state of the art hearing instrument. The Oticon hearing aids that were chosen for Abigail, the VIGO PRO, cost approximately $2000 per hearing aid. This makes our total about $3600 for her aids alone.
The cost of an ear mold impression ranges from about $80 USD to $175 USD depending on the material that the ear mold is constructed from. The cost is constructed of two sub costs--the cost of the actual impression being taken by an audiologist and the cost that the company charges for the construction of the ear mold. Dayton Childrens' Audiology department sends their ear mold impressions to a company in Pennsylvania called Microsonic. The cost of Abby's ear molds are $100 a piece, bringing our grand total for ear molds and aids to $4200.
Although the financial cost was overwhelming to us, we were certain that our insurance would be there for our daughter and help pay a portion of the cost. This is where our caseworker began to explain that most insurance providers do not pay for hearing aids, regardless of whether they are for children. I found this fact absolutely appalling and plan on writing more about this later on, but lucky for us we had one of the few insurance providers that paid for hearing aids in full. The only stipulation is that the child must possess a hearing loss significant enough to affect proper speech development. We would not be required to pay any portion of her hearing aids, which was a relief to us.
Since we an Active Duty Air Force family we have the military insurance program, Tricare. While most Active Duty families have free healthcare at military treatment facilities, we have chosen to pay out of pocket for a more PPO style Tricare program. However, it wouldn't have mattered which Tricare option we had chosen because Tricare is one of the few insurance providers that pay for hearing aids. In the next post I will talk about Ohio's state funded program, BCMH, that can help parents of deaf and HOH children whose insurance does not provide the same financial help that we were lucky to have.
Shortly after Abigail's HOH diagnosis we had a meeting with our caseworker to discuss our insurance and how we intended to fund the purchase of Abigail's hearing aids. Since Abigail has a bilateral loss (a hearing loss in both ears) we would be purchasing two hearing aids in addition to two ear molds (click here for an interesting article on ear molds). Hearing aids range in price from $1000 USD for a quality basic hearing aid to over $3000 USD for a state of the art hearing instrument. The Oticon hearing aids that were chosen for Abigail, the VIGO PRO, cost approximately $2000 per hearing aid. This makes our total about $3600 for her aids alone.
The cost of an ear mold impression ranges from about $80 USD to $175 USD depending on the material that the ear mold is constructed from. The cost is constructed of two sub costs--the cost of the actual impression being taken by an audiologist and the cost that the company charges for the construction of the ear mold. Dayton Childrens' Audiology department sends their ear mold impressions to a company in Pennsylvania called Microsonic. The cost of Abby's ear molds are $100 a piece, bringing our grand total for ear molds and aids to $4200.
Although the financial cost was overwhelming to us, we were certain that our insurance would be there for our daughter and help pay a portion of the cost. This is where our caseworker began to explain that most insurance providers do not pay for hearing aids, regardless of whether they are for children. I found this fact absolutely appalling and plan on writing more about this later on, but lucky for us we had one of the few insurance providers that paid for hearing aids in full. The only stipulation is that the child must possess a hearing loss significant enough to affect proper speech development. We would not be required to pay any portion of her hearing aids, which was a relief to us.
Since we an Active Duty Air Force family we have the military insurance program, Tricare. While most Active Duty families have free healthcare at military treatment facilities, we have chosen to pay out of pocket for a more PPO style Tricare program. However, it wouldn't have mattered which Tricare option we had chosen because Tricare is one of the few insurance providers that pay for hearing aids. In the next post I will talk about Ohio's state funded program, BCMH, that can help parents of deaf and HOH children whose insurance does not provide the same financial help that we were lucky to have.
Pink Hearing Aids?
Friday, January 2, 2009
The ENT gave us the medical clearance for hearing aids, so we headed back to the audiologist to get busy learning all about our options. Abigail's hearing loss falls in the moderate-severe range so we believe that she will benefit greatly from aids. We had little to no input on what hearing aids Abigail would be receiving. At first, I was slightly annoyed--Why shouldn't we choose the aids or at least be asked our opinion. However, this feeling quickly faded when I realized that I know absolutely nothing about hearing aids, or even how our ears work. Once our audiologist started explaining all the benefits of the hearing aids that she would receive, I was confident in her ability to choose the best aid devices for our daughter. The features were all so technical that I truly was relieved that she had done all the research for us and picked the perfect aids.
Abigail would receive the Oticon Vigo Pro, a hearing aid perfect for infants. It has several nice features for little ones to grow with. It has the ability to have an optional wireless FM boot, it has no external on/off switch to prevent little hands from turning off their aids by themselves, it has smart technology to amplify the sounds you want to hear while dampening background noise.
The only choice we had left to make was the color! I thought long and hard about this because our insurance only pays for our hearing aids once every four years unless there is a medically necessary reason for upgrading (I plan on talking about insurance in a future post). The Vigo Pro comes in 10 different colors including skin colors. I originally thought that I would pick skin color aids so that they wouldn't be as noticeable, but the more I thought about it, the more I wanted them to be a sign of pride for her. I want her to love them, to want to wear them, to consider them a cute accessory that she can't wait to put on! That's when it hit me, I decided on soft pink ice--a pearlized baby pink. I hope that she will love them and that they will be a perfect addition for her!
Abigail would receive the Oticon Vigo Pro, a hearing aid perfect for infants. It has several nice features for little ones to grow with. It has the ability to have an optional wireless FM boot, it has no external on/off switch to prevent little hands from turning off their aids by themselves, it has smart technology to amplify the sounds you want to hear while dampening background noise.
The only choice we had left to make was the color! I thought long and hard about this because our insurance only pays for our hearing aids once every four years unless there is a medically necessary reason for upgrading (I plan on talking about insurance in a future post). The Vigo Pro comes in 10 different colors including skin colors. I originally thought that I would pick skin color aids so that they wouldn't be as noticeable, but the more I thought about it, the more I wanted them to be a sign of pride for her. I want her to love them, to want to wear them, to consider them a cute accessory that she can't wait to put on! That's when it hit me, I decided on soft pink ice--a pearlized baby pink. I hope that she will love them and that they will be a perfect addition for her!
Subscribe to:
 Posts (Atom)
Posts (Atom)

{kind=link}